




















































Three Subtypes of Severe Pneumonia Might Inform Personalized Therapies

The results of a study headed by researchers at the University of Cambridge suggest that severe pneumonia has three different subtypes, a discovery that could help to explain why some patients in intensive care units (ICUs) recover from their illness faster than others, and for some patients, the disease can be life-threatening. Rather than assessing patients’ symptoms, the Cambridge team analyzed fluid taken from the lungs of patients admitted to the hospital with suspected pneumonia. Their results indicated that although each of the three different “pneumotypes” of severe pneumonia was associated with how the patients recovered, none could be reliably identified using standard blood tests.
The researchers suggest that their findings could in the future help inform personalized therapeutic strategies, allowing individual patients to receive the most appropriate treatment. Andrew Conway Morris, PhD, at the Department of Medicine at the University of Cambridge and an ICU consultant at Addenbrooke’s Hospital, Cambridge, is senior author of the team’s published paper in Nature Communications, titled “Pulmonary inflammation in severe pneumonia is characterised by compartmentalised and mechanistically distinct sub-phenotypes.”
Pneumonia is the commonest infectious cause of death worldwide, responsible for an estimated 2.5 million deaths per year, the researchers noted. In severe cases, patients may need to be admitted to an ICU and given mechanical ventilation. Severe pneumonia accounts for six in 10 infections managed in intensive care, and spread of the infection within ICUs is a significant concern.
Doctors have long struggled to understand why patients whose condition looks similar clinically can have very different recoveries. Some respond quickly to treatment, while others remain critically ill for weeks or even die. “Despite the considerable burden of pneumonia, the syndrome is incompletely understood, and diagnosis is difficult,” the team explained.
Conway Morris said, “Even though we’re able to treat the initial infection, many patients with severe pneumonia still struggle to come off the ventilator and can develop lung failure. Therapies to tackle inflammation in the lungs have had mixed results in clinical trials—some suggest they are beneficial, others that they’re harmful.”
Severe pneumonia is usually diagnosed through a combination of symptoms, imaging, and blood tests. Symptoms typically include fever or hypothermia, low oxygen levels, breathing difficulties, and confusion. “The current approach of classifying patients by their clinical syndromes—sepsis, acute respiratory distress syndrome, and so on—without looking at the underlying biology risks missing what’s key,” Conway Morris noted. “Instead of asking ‘Does this patient have pneumonia?’, we should be asking ‘What’s the inflammatory pattern in this patient’s lungs?’”
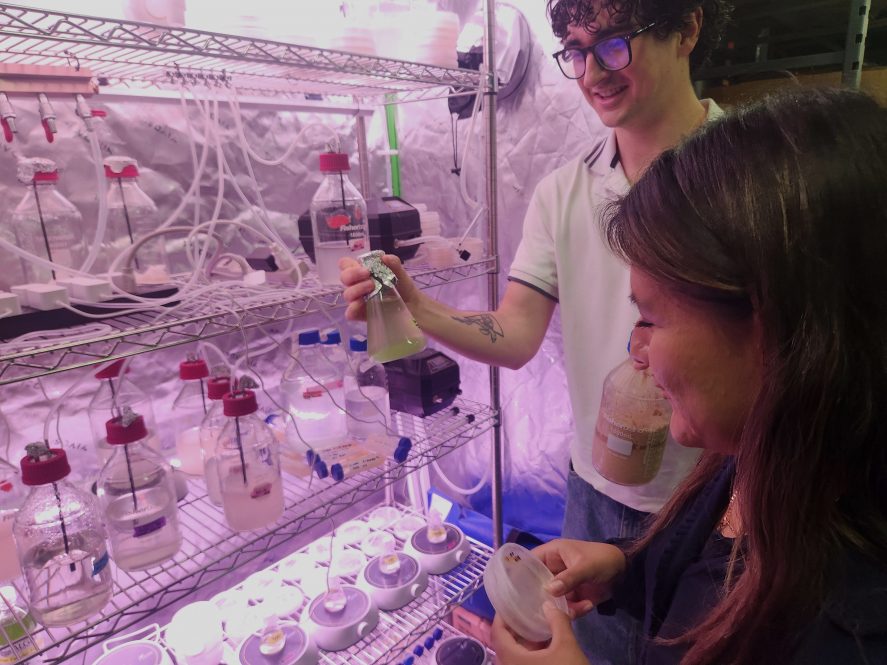
For their newly reported study, Conway Morris and team recruited 80 patients admitted with suspected severe pneumonia to the ICU at Addenbrooke’s Hospital. Instead of relying only on blood tests or scans, however, the Cambridge team analyzed the patient’s immune cells, inflammatory signals, and gene activity in bronchoalveolar lavage samples. “Here, we perform multifaceted assessments of bronchoalveolar transcriptome, cytokines, microbiology, and clinical features to biologically characterise a cohort of patients with suspected severe pneumonia,” they reported in their paper. The researchers discovered three distinct biological types—or pneumotypes (Pn)—of severe pneumonia, none of which could be reliably detected using standard blood tests, even though they were strongly linked to how patients recovered.
“Using bulk RNA sequencing of bronchoalveolar fluid, we have identified three phenotypes in the lungs of patients with lung injury and suspected pneumonia,” they stated. “These phenotypes were reflected in the differential immune cell populations and inflammatory proteins.”
The most common pneumotype—accounting for almost half (49%) of cases—was characterized by immune suppression, significant damage to the lining of the lungs, and bleeding in the alveoli (tiny air sacs within the lungs). There were fewer signs of inflammation, which may explain why treatments targeting inflammation can fail or even harm some patients. “Pn1, the most common, is characterized by low alveolar cytokines, expanded tolerogenic macrophages, and epithelial damage,” the investigators reported.
The second pneumotype—accounting for just under a quarter (23%) of cases—was characterized by a balanced immune response and active repair of damage to the lungs. Patients were most likely to recover faster from this pneumotype and require the shortest time on the ventilator, even though they initially looked just as ill as the others. “Pn2 displays the fastest resolution, exhibiting a balanced immune response and epithelial-endothelial repair signatures,” they continued.
Patients with the most dangerous pneumotype—the one that most resembles “classic” pneumonia—spent the longest on mechanical ventilation and had prolonged critical illness. They had severe and persistent inflammation, with a flood of immature immune cells in the lung. This group may be most likely to respond to anti-inflammatory therapies, the team said. “Pn3 is characterized by immature neutrophil infiltration, IL-6-STAT3 activation, and longer duration of mechanical ventilation,” the scientists stated.
First author Dr. Mark Jeffrey, at the Department of Medicine at the University of Cambridge, added, “Even though on the surface, all of the patients seemed to have similar types of pneumonia, with comparable illness severity, oxygen levels, and clinical diagnoses, their outcomes were very different. It was only when we drilled down and looked at patterns of inflammation that the differences became apparent. Severe pneumonia is not a single disease, but several biologically distinct conditions that happen to look alike. This helps explain why ‘one-size-fits-all’ treatments—including some immune-modulating drugs—have often failed in clinical trials.”
Interestingly, the authors added in their report, “Each of the Pneumotypes contained both patients with and without confirmed pneumonia, implying common mechanisms underpinning lung injury arising from different mechanisms.”
The tests used to determine the pneumotypes are too complex to enable rapid classification, but the researchers hope to develop a simplified tool that could help them stratify the patients and ultimately offer tailored treatments.
Co-author Vilas Navapurkar, MBChB, from the John Farman Intensive Care Unit at Addenbrooke’s Hospital, said, “If we know which subtype of pneumonia an individual has, we can potentially tailor their treatment more precisely, boosting the immune response in some, while calming harmful inflammation in others. This has the potential to help critically ill patients, reduce deaths from pneumonia, shorten ICU stays, and cut unnecessary antibiotic use.”
The team also noted that while their study identified three Pneumotypes, it’s likely that others may exist, which might be identified in larger studies. In conclusion, they wrote, “… we have identified and validated three pulmonary confined endotypes in patients with severe pneumonia and lung injury. These phenotypes are underpinned by distinct mechanisms and have differential outcomes. The mechanisms point to different therapeutic options, as well as extending our understanding of the biology of lung inflammation in the context of severe pneumonia.”
The post Three Subtypes of Severe Pneumonia Might Inform Personalized Therapies appeared first on GEN - Genetic Engineering and Biotechnology News.
Apa Reaksi Anda?
 Suka
0
Suka
0
 Kurang Suka
0
Kurang Suka
0
 Setuju
0
Setuju
0
 Tidak Setuju
0
Tidak Setuju
0
 Bagus
0
Bagus
0
 Berguna
0
Berguna
0
 Hebat
0
Hebat
0